Intended for healthcare professionals
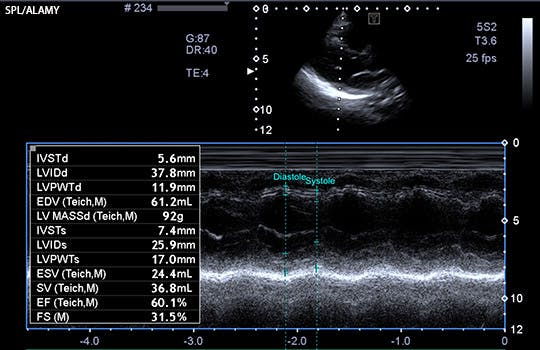
Predicting the risks of kidney failure and death in adults with moderate to severe chronic kidney disease


TRIPOD+AI: an updated reporting guideline for clinical prediction models
The new TRIPOD+AI guideline incorporates recent advances in clinical prediction modelling, notably in the realm of machine learning
TRIPOD+AI: an updated reporting guideline for clinical prediction models
The new TRIPOD+AI guideline incorporates recent advances in clinical prediction modelling, notably in the realm of machine learning

Refocusing the WHO’s Model List of Essential Medicines on the needs of low and middle income countries
In the wake of escalating medicine prices, Veronika Wirtz and colleagues argue for change
Refocusing the WHO’s Model List of Essential Medicines on the needs of low and middle income countries
In the wake of escalating medicine prices, Veronika Wirtz and colleagues argue for change

Alternative routes into clinical research: a guide for early career doctors
This article outlines the “non-traditional” routes that can enable research-active careers
Alternative routes into clinical research: a guide for early career doctors
This article outlines the “non-traditional” routes that can enable research-active careers
New death certification process for England and Wales will start in September
Why the fuss about physician associates?
Mortality in working age people is still significantly higher than pre-pandemic, data show
NHS England does U turn on staff mental health service after outcry by doctors
How can I deal with the death of a patient?
NHS and the whole of society must act on social determinants of health
Sustainability is critical for future proofing the NHS
Latest articles
News

Breast cancer: Inaction on inequalities has led to unequal progress, say experts
Most members on FDA advisory panel that recommended cardiac device had received payments from its maker
Deaths of despair are higher among black and Native Americans, study finds
Sixty seconds on . . . the eclipse
Paediatric waiting lists in Northern Ireland are a “catastrophe,” say doctors
Almost a third of UK doctors are considering moving abroad soon, survey suggests
Covid-19: Charities question inquiry’s “refusal” to fully examine mental health impact
Haytox: what is the evidence for a Botox spray for hay fever?
French government gives go-ahead to voluntary assisted dying
Research

Impact of large scale, multicomponent intervention to reduce proton pump inhibitor overuse
Glucagon-like peptide 1 receptor agonist use and risk of thyroid cancer
Quantifying possible bias in clinical and epidemiological studies with quantitative bias analysis: common approaches and limitations
Use of progestogens and the risk of intracranial meningioma
Delirium and incident dementia in hospital patients
Derivation and external validation of a simple risk score for predicting severe acute kidney injury after intravenous cisplatin
Quality and safety of artificial intelligence generated health information
Large language models and the generation of health disinformation
Comment

Sudan is facing a devastating humanitarian crisis—the world must do more to protect the population’s health
Planetary health: challenging power and privilege is key to a fairer and healthier future
Choosing Wisely in a time of resource constraints
How on earth did I miss that?
Invisibility and discrimination harm women from ethnic minorities working in the NHS
Scarlett McNally: Small changes for better use of time and teams
Striking racial inequities in health persist in South Africa
Gender medicine for children and young people is built on shaky foundations
Recognising the huge gains for all from liberating girls and women
Education
Advances in management of heart failure
Non-acute heart failure management in primary care
Group A beta-haemolytic streptococcal infection in children
Secondary prevention of cardiovascular disease, including cholesterol targets: summary of updated NICE guidance
Effectiveness and safety of drugs for obesity
Dry eye disease management
Caring is the invisible piece of the stroke recovery puzzle
Stroke rehabilitation in adults: summary of updated NICE guidance
How to make the most of your ophthalmology placement
Premature ovarian insufficiency
Workforce


BMJ Medicine

Practical implications of the ADNEX risk prediction model for diagnosis of ovarian cancer
Apr 3
Socioeconomic inequalities in risk of infection with SARS-CoV-2 delta and omicron variants in the UK, 2020-22
Mar 11
Preterm prelabour rupture of membranes before 23 weeks’ gestation
Mar 19
All cause and cause specific mortality associated with transition to daylight saving time in US
Mar 6
UK Jobs
Current issue

Most read
1.
Ultra-processed food exposure and adverse health outcomes: umbrella review of epidemiological meta-analyses
2.
Effect of exercise for depression: systematic review and network meta-analysis of randomised controlled trials
3.
Use of progestogens and the risk of intracranial meningioma: national case-control study
4.
Rosuvastatin versus atorvastatin treatment in adults with coronary artery disease: secondary analysis of the randomised LODESTAR trial
5.
Delirium and incident dementia in hospital patients in New South Wales, Australia: retrospective cohort study
6.



